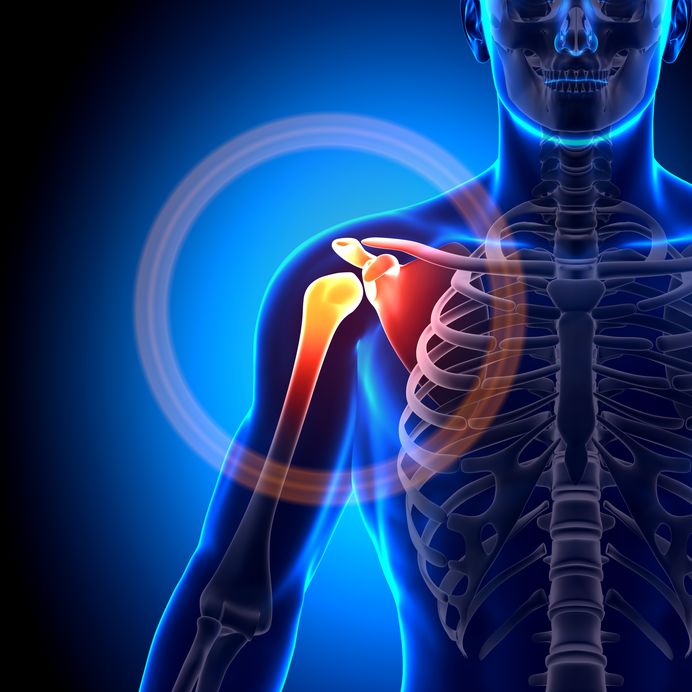
Shoulder Pain A comfortable shoulder is essential for everyday life and sports. The shoulder region includes the collarbones, chest muscles,…

Neck Pain A comfortable neck is essential for everyday life and sports. The anatomy of the neck includes the muscles,…

Back Pain A comfortable low back is essential for everyday life and sports. Back pain is a very common symptom…

A brief history…. Introduction Cancer rehabilitation is highly valued by people who have cancer diagnoses and the evidence is mounting…
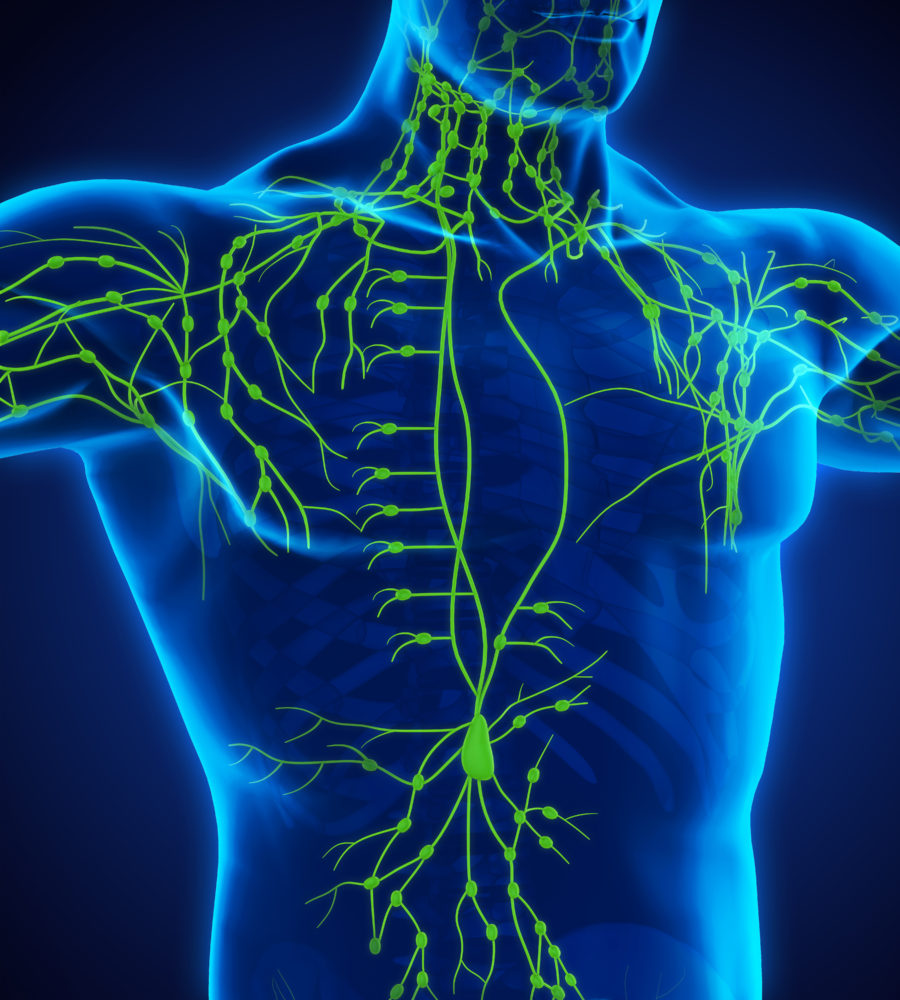
Lymphoedema is an abnormal accumulation of protein-rich fluid (oedema ) in the interstitium most often in the arm(s) and/or leg(s),…

TRAM Flap and Physio. A flap of the woman’s own tissue is used to reconstruct a natural feeling and looking…

Breast cancer Rehab for Physiotherapists Course This article “Sex therapy after cancer” by Relationships Ireland was approved for the course…
Breast Cancer Rehabilitation For Physiotherapists Updated October 2016. Written by Siobhan O’ Reilly Bracken MISCP PT MPA MSc CLT. Email…
